
Golfer’s Elbow can present a frustrating challenge for anyone who experiences it, whether they are a professional athlete, an enthusiastic golfer, or someone engaged in daily activities that strain the arm. Many individuals find that pain at the inside of the elbow disrupts both their performance and their overall quality of life. Understanding how Golfer’s Elbow develops and what it involves is crucial in managing it effectively and preventing its recurrence.
Golfer’s Elbow is not exclusive to golfers. People who frequently grip, lift, or swing objects, such as tennis players, bowlers, gardeners, and even those lifting heavy objects at work, may experience similar symptoms. The term “Golfer’s Elbow” arises simply because this condition is often seen in individuals who play golf, where repetitive wrist and forearm motions can irritate structures in the inner elbow.
What Is Golfer’s Elbow
Golfer’s Elbow is a condition involving pain, irritation, or tenderness on the inner side of the elbow. It is medically referred to as medial epicondylitis, indicating inflammation or micro-tearing of the tendons that attach to the medial epicondyle of the humerus (the bony knob on the inside of the elbow). This problem can stem from acute overuse or chronic strain on these tendons, often causing significant discomfort and functional impairment in the arm and hand.
People with Golfer’s Elbow frequently notice symptoms while gripping objects, twisting their forearm, or flexing their wrist against resistance. The hallmark sign is usually localized pain near the inside of the elbow that can radiate down the forearm. With early diagnosis and appropriate treatment, Golfer’s Elbow can often be managed effectively, minimizing the risk of more severe complications.
Anatomy of the Golfer’s Elbow
Understanding the anatomical structures involved in Golfer’s Elbow is key to recognizing why specific movements or tasks trigger pain.
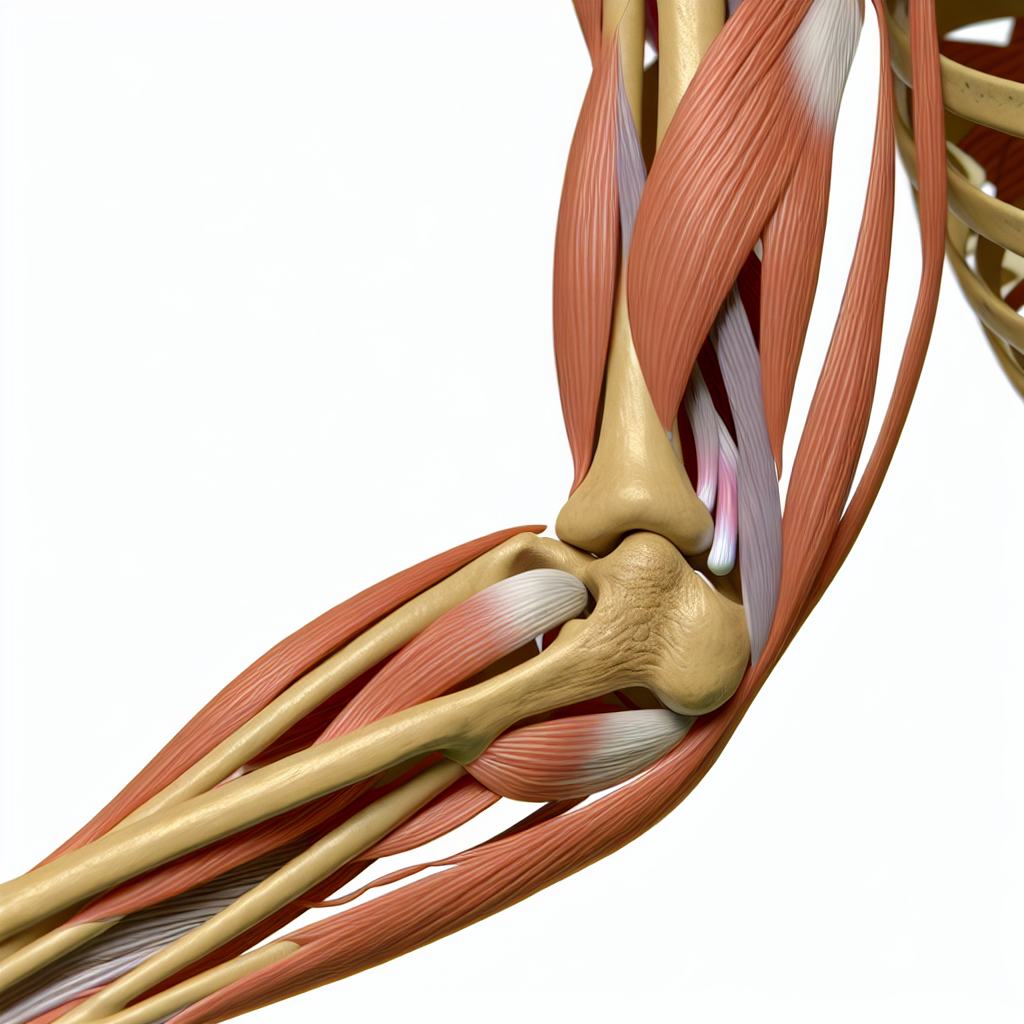
- Medial Epicondyle
This bony prominence lies on the inner side of the lower humerus (upper arm bone). It serves as an attachment point for several tendons responsible for wrist and finger flexion. - Wrist Flexors and Pronator Muscles
Muscles like the pronator teres, flexor carpi radialis, flexor carpi ulnaris, and flexor digitorum superficialis originate around the medial epicondyle. When these muscles contract, they enable the wrist and fingers to flex (bend) and assist in pronation (turning the palm downward). - Tendons
Tendons connect muscles to bones. In Golfer’s Elbow, the tendons on the medial side of the elbow experience small tears or degeneration where they attach to the medial epicondyle, leading to inflammation and pain. - Ulnar Collateral Ligament (UCL)
This ligament supports the inner side of the elbow joint and may sometimes be irritated or stressed in individuals with Golfer’s Elbow, although it is not always directly involved.
When repetitive stress and microtrauma occur in these tissues, Golfer’s Elbow can emerge, causing localized tenderness and reduced tolerance for movements that load these structures.
What Causes Golfer’s Elbow?
Golfer’s Elbow often results from repetitive or excessive strain on the wrist flexor and pronator muscles near the inner elbow. While golfing can be a common culprit, many other activities can lead to similar repetitive stress:
- Frequent, forceful gripping or lifting
- Incorrect sports techniques (e.g., improper swing in golf or tennis)
- Occupational tasks that require continuous wrist flexion or hammering
- Sudden increase in activity intensity without proper conditioning
- Poor ergonomics in daily tasks or while using a computer
These factors gradually place more tension on the medial structures of the elbow than they can withstand, resulting in micro-tears. If the body does not receive adequate rest and recovery time, inflammation and pain persist.
Short bursts of extreme force or changes in technique can also damage the tendons. For instance, an abrupt transition from an off-season period of inactivity to an intense practice schedule may overwhelm the tissues in the forearm. In each case, the core problem remains the chronic overuse and insufficient recovery of the wrist flexor tendons that attach to the medial epicondyle.
What Are the Symptoms of Golfer’s Elbow?
Individuals suffering from Golfer’s Elbow typically report distinct yet sometimes overlapping symptoms. Identifying these early can guide timely intervention and prevent more severe complications:
- Pain or tenderness on the inside (medial side) of the elbow
- Discomfort that may radiate down the inner forearm
- Stiffness or reduced mobility in the elbow and wrist
- Weak grip strength or difficulty grasping objects
- Pain aggravated by wrist flexion, pronation, or gripping tasks
- Possible swelling, though not always prominent
The level of discomfort can vary from a mild annoyance to a sharp, persistent pain that interferes with daily activities. Some people notice a dull ache at rest, while others feel pain only when attempting certain movements.
Special Test of Golfer’s Elbow
Several clinical tests help confirm Golfer’s Elbow by reproducing its characteristic pain in a controlled manner. Although these tests can guide diagnosis, a thorough clinical evaluation, including history-taking and imaging (if needed), is essential.
Resisted Wrist Flexion Test
- The individual sits or stands with the elbow extended and the forearm supinated (palm facing upward).
- The examiner stabilizes the forearm and asks the individual to flex the wrist against resistance.
- Pain at the medial epicondyle region during this action suggests Golfer’s Elbow.
Resisted Forearm Pronation Test
- The individual starts with the elbow at 90 degrees of flexion and the forearm in a neutral or slightly supinated position.
- The examiner stabilizes the elbow and asks the individual to pronate (turn the palm downward) against resistance.
- Medial elbow pain indicates possible irritation of the muscles that attach to the medial epicondyle.
Palpation of the Medial Epicondyle
- The examiner gently palpates the medial epicondyle area.
- Tenderness or discomfort, especially if localized to the tendon origin, may confirm the presence of inflammation associated with Golfer’s Elbow.
Golfer’s Elbow Stress Test
- The elbow is extended, and the examiner passively extends the wrist and fingers, placing stress on the medial elbow structures.
- If this maneuver reproduces the individual’s familiar inner elbow pain, it supports the diagnosis.
These tests aim to systematically reproduce the stresses on the tendons that cause Golfer’s Elbow discomfort. A positive result often guides clinical management and indicates that the medial elbow tissues require focused intervention.
How Do We Treat Golfer’s Elbow
Many people find relief from Golfer’s Elbow by combining self-management strategies with professional guidance. Treatment should target both the symptoms and their underlying causes, ensuring a longer-term resolution.
- Rest and Activity Modification
Temporarily reducing or stopping activities that aggravate the elbow can help reduce inflammation. Instead of complete inactivity, light exercises or alternative activities that avoid overstressing the medial elbow can maintain overall fitness without worsening the condition. - Pain Management
Local ice application helps relieve acute discomfort and inflammation. Anti-inflammatory medications may be beneficial in the short term for severe pain or swelling. However, always consult a healthcare professional regarding medication. - Physiotherapy Exercises
Targeted exercises form the backbone of Golfer’s Elbow rehabilitation. Gentle stretching, muscle-strengthening routines, and progressive loading of the wrist flexors support tendon healing and help prevent re-injury. Eccentric exercises, where muscles lengthen under tension, are highly valued for tendon recovery. - Bracing or Support
A counterforce brace or elbow strap worn around the forearm can alleviate tension at the medial epicondyle. Proper sizing and placement are crucial for its effectiveness, and it should be combined with other management strategies, not used alone as a permanent solution. - Gradual Return to Activity
Once symptoms decrease, a gradual reintroduction of sports or occupational tasks is key. This phased approach ensures that the healing tissues can adapt to increased loads without a flare-up.
By focusing on reducing aggravating factors and employing appropriate exercises, many people recover from Golfer’s Elbow and return to their usual activities. Early intervention typically improves outcomes and shortens recovery times.
Golfer’s Elbow Treatment Approaches
A variety of treatment options exist for Golfer’s Elbow, and the best approach often involves a combination of techniques. Physiotherapists select and tailor interventions based on each individual’s condition and goals.
Exercise-Based Rehabilitation
- Flexibility Work
Gentle stretching of the wrist flexors and extensors helps restore normal range of motion and prevents tightness from persisting in the area. Painless stretching can be done multiple times a day to gradually ease tension. - Progressive Strengthening
Exercises targeting the forearm muscles, especially the wrist flexors and pronators, are incrementally progressed. Light resistance bands or small dumbbells are commonly used to restore strength. Eccentric loading (slowing lengthening of the forearm muscles during exercise) is especially beneficial for tendon healing. - Grip and Functional Training
Activities that incorporate grip strength and dexterity can help individuals return to the functional tasks or sports they love. Therapists might introduce putty exercises, ball squeezes, or specific hand movements to help re-establish normal function.
Manual Therapy
- Soft Tissue Mobilization
Techniques such as myofascial release, cross-friction massage, or trigger point therapy may help reduce adhesions and improve tendon pliability. By targeting the medial elbow region, a therapist aims to enhance local circulation and decrease tension. - Joint Mobilization
Gentle joint mobilization of the elbow or surrounding joints in the upper extremity can help improve overall arm mechanics and reduce abnormal stress on the medial epicondyle.
Modalities
- Ultrasound
Therapeutic ultrasound delivers sound waves to deeper tissues, aiding in pain relief and promoting circulation. It may also facilitate tissue healing when applied with the correct parameters. - Laser Therapy
Low-level laser therapy can help with tendon healing and pain reduction by improving cellular activity in the affected area. - Electrical Stimulation
Techniques like transcutaneous electrical nerve stimulation (TENS) can alleviate pain by stimulating nerves and interrupting pain signals, often providing short-term relief.
Injection Therapies
- Corticosteroid Injection
In cases of severe pain unresponsive to conservative care, a corticosteroid injection may offer relief by reducing inflammation. However, repeated injections should be approached with caution due to potential side effects on tendon integrity. - Platelet-Rich Plasma (PRP)
PRP injections use concentrated platelets from the individual’s own blood to encourage tendon healing. Though results can vary, this approach has shown promise in treating persistent tendinopathies.
Surgical Intervention
Most individuals improve with conservative management, but surgery can be considered in cases where chronic Golfer’s Elbow fails to respond to all other treatments. Surgical options might involve removing damaged tissue and reattaching healthy tendons to the medial epicondyle. Rehabilitation post-surgery can be extensive, and recovery times vary.
Golfer’s Elbow Differential Diagnosis
When diagnosing Golfer’s Elbow, it is crucial to distinguish it from other potential sources of inner elbow pain:
- Cubital Tunnel Syndrome (Ulnar Nerve Entrapment)
This condition involves compression of the ulnar nerve around the medial elbow. Symptoms can include numbness or tingling in the ring and little fingers, along with medial elbow discomfort. However, nerve-related symptoms typically present with distinct patterns of tingling or altered sensation. - Medial Collateral Ligament (MCL or UCL) Injury
The ulnar collateral ligament stabilizes the medial elbow. Injuries (particularly in throwing athletes) can present with medial elbow pain, instability, or a feeling of giving way during overhead activities. Unlike Golfer’s Elbow, the pain may be more ligament-related, especially with valgus stress. - Referred Pain from the Cervical Spine
Sometimes, nerve irritation in the neck or other structures in the shoulder region can refer pain to the medial elbow. A thorough clinical examination helps rule out these regions when diagnosing Golfer’s Elbow. - Elbow Joint Pathologies
Intra-articular issues such as osteoarthritis, loose bodies, or synovial plica may cause localized pain. Although the medial side can be affected, these conditions often have broader joint involvement and different clinical signs upon examination.
Proper evaluation and imaging, where necessary, ensure an accurate diagnosis. This process prevents misdiagnosis and guides effective treatment strategies, ensuring the person receives the most suitable care for their condition.
Golfer’s Elbow Prognosis and Expectations
Golfer’s Elbow can often resolve with proper management, particularly if treatment is initiated early and tailored to the individual’s specific needs. A combination of activity modification, targeted exercises, and possible adjunct therapies can significantly improve outcomes. However, recovery timelines vary based on factors such as the severity of tendon damage, compliance with rehabilitation, and any coexisting issues.
- Short-Term Outlook
With consistent conservative treatment, many individuals experience a significant reduction in pain within a few weeks. Early intervention can help quickly mitigate inflammation and prevent chronic complications. - Long-Term Expectations
Most individuals return to full participation in sports or daily routines if they adhere to recommended rehabilitation guidelines. Persistent discomfort or recurrent flare-ups may indicate that the tendons are still healing or that underlying biomechanical issues have not been addressed. - Prevention of Recurrence
Ongoing strengthening and flexibility exercises should continue even after symptoms resolve. Proper technique in sports or work-related tasks, regular breaks, and awareness of overuse patterns can help prevent Golfer’s Elbow from returning.
Throughout recovery, open communication with healthcare professionals ensures that the rehabilitation program remains focused and adaptable. Adequate rest, gradual progression of activities, and a strong emphasis on prevention strategies set the stage for a positive prognosis and a swift return to pain-free motion.
By carefully considering each aspect of Golfer’s Elbow—from its causes to its clinical presentation, assessment, and management—individuals can enhance their understanding of how best to tackle this condition. Whether through early activity modification, structured physiotherapy, or, in rare cases, surgery, appropriate interventions can effectively address the pain and support a healthy, active lifestyle.